I hitched a ride with Terry to day who works in Philly and does this terrible commute everyday of his life. He came up to Danny’s room to say hi. We turned the corner and there was danny sitting in bed with the tube back up his nose.
I hitched a ride with Terry to day who works in Philly and does this terrible commute everyday of his life. He came up to Danny’s room to say hi. We turned the corner and there was danny sitting in bed with the tube back up his nose.
“What happened?” I said.
“There was so much blood. The guy didn’t know what he was doing. He just kept pushing it in and he making me bleed. He couldn’t get around the curve in the back of my nose. Blood was pouring out. So he pulled out and tried the other nostril and still couldn’t get it. I told him he had to stop. He said he had an idea.I said- YOU HAVE AN IDEA?. AN IDEA? Haven’t you ever done this before?
You got a short, thicker tube and jammed in in my nose to get around the curve and then fed the smaller tube down into my stomach. There was so much blood. I vomited. I feel sick.” said danny with a hoarse strained voice.
The clear liquid diet he was allowed yesterday wasn’t digested by his traumatized stomach and just laid in there making him sicker. Now they had to put the tube back in to suck out all the liquids and gastric juice his body makes until his lazy ole stomach wakes up. He is still in pain but he doesn’t want to use any morphine because he doesn’t want that sluggish stomach to be all drugged up. I told the nurse on him because I know if your body has to be dealing with pain and healing it is too much. You NEED pain meds to heal. Its true that you don’t want to use too much and it does slow all your body down. You just have to find a good balance.
He said he was so happy I came in early because he really needed me there. I knew he did. I can feel is emotions even from long distances. I think tomorrow I will drive myself in so I can be sure to get there early. I hate driving in the city, but when someone needs you, you do whatever you got to do.
Needless to say he was not a happy camper yesterday. He kind of looked like an elephant with that thing coming out of his nose. A resident doctor came in and took one look at it and said, “Its in too far, we have to X-ray.” The nurse said, “No it’s fine, he’s just a tall guy.” While the resident was there he took out one of Danny’s drains. He has two. One less tube ! Wahoo!
They took Danny down for an X-ray. Sonnet, Kevin,me and the kids went to the Reading Terminal market for lunch while they worked on Danny.I got my lunch to go and went back to the hospital leaving everyone else at the market. Danny returned with a new tube.The old tube was coiled up in his stomach which was causes additional pain. Danny was pissed. They pulled it out and fixed it. He got about a 10 minute rest and then they took him to physical therapy to work out. He walked, did a scary obstacle course, up and down stairs and ballet at the bar. hen he got back to his room he walked some more. They want him to walk as much as he can, which is still pretty hard since he’s connected to fifty million tubes.
Sonnet and the kids returned but Ana and Ry just bickered the whole time so Sonnet decided to just take the brats home. Danny was in no mood for fighting children. Bad babies, bad! Lerin came then and that made Danny smile. It was probably his only smile of the day.

What is That tube in his nose?
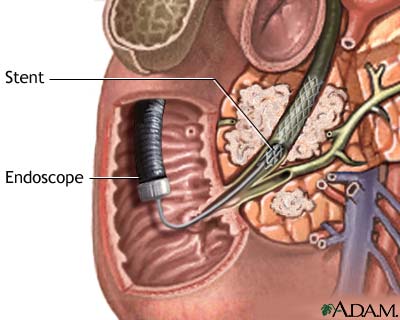
Nasogastric aspiration (suction) is the process of draining the stomach’s contents via the tube. Nasogastric aspiration is mainly used to remove gastric secretions. It can also be appended to a suction system, however this method is often restricted to emergency situations, as the constant suction can easily damage the stomach’s lining. In non-emergent situations, intermittent suction may be applied giving the benefits of suction without the untoward effects of damage to the stomach lining.
Before an NG tube is inserted, it must be measured from the tip of the patient’s nose, loop around their ear and then down to roughly 5 cm below the xiphoid process. The tube is then marked at this level to ensure that the tube has been inserted far enough into the patient’s stomach. Many commercially available stomach and duodenal tubes have several standard depth markings, for example 18″ (46 cm), 22″ (56 cm), 26″ (66 cm) and 30″ (76 cm) from distal end; infant feeding tubes often come with 1 cm depth markings. The end of a plastic tube is lubricated (local anesthetic, such as 2% xylocaine gel, may be used; in addition, nasal vasoconstrictor and/or anesthetic spray may be applied before the insertion) and inserted into one of the patient’s anterior nares. The tube should be directed straight towards the back of the patient as it moves through the nasal cavity and down into the throat. When the tube enters the oropharynx and glides down the posterior pharyngeal wall, the patient may gag; in this situation the patient, if awake and alert, is asked to mimic swallowing or is given some water to sip through a straw, and the tube continues to be inserted as the patient swallows. Once the tube is past the pharynx and enters the esophagus, it is easily inserted down into the stomach. The tube must then be secured in place to prevent it from moving.
Great care must be taken to ensure that the tube has not passed through the larynx into the trachea and down into the bronchi. To ensure proper placement it is recommended (though not unequivocally confirmed) that injection of air into the tube be performed, if the air is heard in the stomach with a stethoscope, then the tube is in the correct position. Another more reliable method is to aspirate some fluid from the tube with a syringe. This fluid is then tested withpH paper (note not litmus paper) to determine the acidity of the fluid. If the pH is 5.5 or below then the tube is in the correct position. If this is not possible then correct verification of tube position is obtained with an X-ray of the chest/abdomen. This is the most reliable means of ensuring proper placement of an NG tube.Future techniques may include measuring the concentration of enzymes such as trypsin, pepsin, and bilirubin to confirm the correct placement of the NG tube. As enzyme testing becomes more practical, allowing measurements to be taken quickly and cheaply at the bedside, this technique may be used in combination with pH testing as an effective, less harmful replacement of X-ray confirmation. If the tube is to remain in place then a tube position check is recommended before each feed and at least once per day.